Chapter 8: Federal Suicide Prevention Resources
Introduction
Collaboration has been a key theme throughout this guide. Just as every child should have the support of family and others in dealing with life’s challenges, every community should have help in promoting the mental health and well-being of its members. The Substance Abuse and Mental Health Services Administration (SAMHSA), as the Federal agency charged with leading national efforts to reduce, prevent, and improve treatment of mental and substance abuse disorders, takes its role in collaboration seriously. As directed by law, Federal mandate, and the compassion of its professionals, SAMHSA is working to provide States and communities with the tools that can help them prevent suicide.
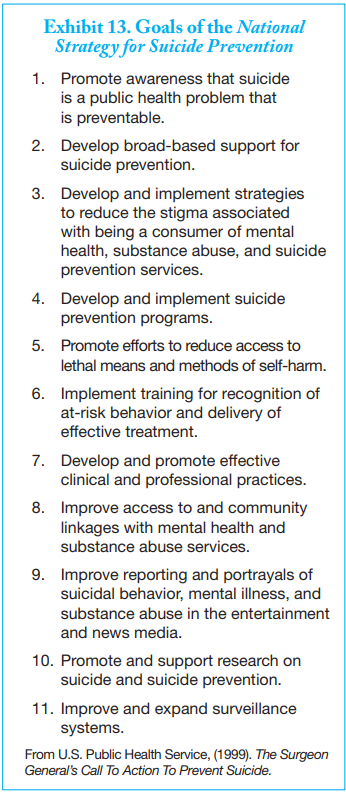
The preceding chapter described suicide prevention programs listed in SAMHSA’s National Registry of Evidence-Based Programs and Practices (NREPP) and its Suicide Prevention Resource Center’s (SPRC’s) Best Practices Registry. This chapter describes SAMHSA programs open to American Indian and Alaska Native (AI/AN) community applicants. It also provides more detail about the SPRC, the National Suicide Prevention Lifeline, and other resources available to AI/AN communities in developing, implementing, and evaluating their suicide prevention plans. All of SAMHSA’s efforts are consistent with the 11 goals of the National Strategy for Suicide Prevention (see Exhibit 13).
The SAMHSA partner in many efforts is the Indian Health Service (IHS). The IHS views such collaboration as essential to its responsibility to uphold the Federal Government’s obligation to promote healthy AI/AN people, communities, and cultures and
to honor and protect the inherent sovereign rights of Tribes. This chapter also lists IHS suicide prevention resources and contact information for IHS regional offices.
Other Federal agencies that may offer possible funding of programs aimed at reducing risk factors related to suicide also are identified.
Suicide Prevention Programs
In 2005, Congress passed the Garrett Lee Smith Memorial Act (GLS) in memory of Garrett Smith, the son of former Senator Gordon Smith, who died by suicide while at college. This Act passed both houses of Congress unanimously.
Under GLS, Congress charged SAMHSA with creating programs to enhance suicide prevention efforts at the State and local level and on college campuses. Since 2005, Congress has placed increasing emphasis on, and given increased funding for, suicide prevention among AI/AN youth and young adults. SAMHSA currently supports suicide prevention grants for AI/AN Tribes and Villages under GLS through its State and Tribal Youth Suicide Prevention and Early Intervention Grant Program, and for AI/AN communities through its Native Aspirations Program.
AI/AN youth also are served as members of a larger population through SAMHSA’s Linking Adolescents at Risk of Suicide to Mental Health Services Grant Program and its Campus Suicide Prevention Grant Program. Additional information about all of SAMHSA’s suicide prevention programs is below.
For up-to-date information on new requests for applications (RFAs), the application process, and due dates for each grant program, consult the grants homepage on the SAMHSA Web site at http://www.samhsa.gov/grants. Information also may be requested from:
Substance Abuse and Mental Health Services Administration
Center for Mental Health Services
Division of Prevention, Traumatic Stress,
and Special Programs
Suicide Prevention Branch
1 Choke Cherry Road
Rockville, MD 20857
State and Tribal Youth Suicide Prevention and Early Intervention Grant Program
This grant program supports States and Tribes in developing and implementing statewide or Tribal suicide prevention and early intervention strategies. Efforts funded by these grants must involve public and private collaboration among youth-serving systems, such as education, juvenile justice, and foster care, as well as substance abuse and mental health service providers.
Grant eligibility is open to:
- States;
- Federally recognized Indian Tribes, Tribal organizations (as defined in the Indian Self-Determination and Educational Assistance Act), or urban Indian organizations (as defined in the Indian Health Care Improvement Act) that are actively involved in the development and continuation of a Tribal youth suicide early intervention and prevention strategy; and
- Public or private nonprofit organizations designated by a State, federally recognized Indian Tribe, Tribal organization, or urban Indian organization to develop or direct the State/Tribal-sponsored youth suicide prevention and early intervention strategy.
Successful applicants must:
- Develop and implement collaborative prevention and early intervention strategies in youth-serving organizations;
- Support public and private organizations actively involved in such efforts;
- Provide early intervention and assessment services to youth who are at risk for mental and emotional disorders that may lead to suicide or a suicide attempt;
- Provide timely referrals for appropriate community mental health care and treatment to youth who are at risk for suicide or suicide attempts;
- Provide immediate support and information resources to families of youth who are at risk for suicide;
- Offer timely post-suicide intervention services, care and information to families, friends, and organizations affected by a recent youth suicide; and
- Participate in data collection and analysis activities and prepare an evaluation report.
Summaries, successes, and contact information from ongoing State and Tribal Suicide Prevention and Early Intervention grants are
available at http://www.sprc.org/grantees/statetribe/desc/S_Tdescriptions.asp
Native Aspirations
In 2005, SAMHSA funded Native Aspirations, a training and technical assistance project that is designed to help AI/AN communities develop, implement, and evaluate a comprehensive, community-based youth violence, bullying, and suicide prevention program. To select eligible communities, the Native Aspirations project team developed a list of high-risk sites based on statistics for poverty, suicide, homicide, and motor vehicle accidents among youth. From that list, behavioral health experts from IHS, Bureau of Indian Affairs, and State programs identified those communities where the need for prevention resources appeared greatest.
For each of its selected communities, Native Aspirations provides consultation and financial support and conducts facilitated events and training to implement a community’s prevention plan. Activities include site visits for project planning, passage of Tribal resolutions or executive orders, and an onsite Gathering of Native Americans (GONA). By providing a safe place to share, heal, and plan for action, the GONA offers hope and a positive start to communities. Additional onsite activities include a youth visioning event to gain youth input and involvement. GONA activities also include a community mobilization and planning event to engage as many stakeholders as possible—including Tribal Elders, youth, and representatives of local youth-serving systems—and to strengthen collaborations across IHS, States, and Native communities.
Native Aspiration grant sites are included in the ongoing cross-site evaluation of State and Tribal Youth Suicide Prevention and Early Intervention sites. Preliminary lessons learned that are applicable to current and future prevention efforts are:
- A grassroots focus is essential when working with Tribal communities;
- Programs and activities need to respond to the unique strengths and barriers that exist within each individual community;
- Program development must be community-driven so that community buy-in and ownership is fostered from the very beginning; and
- Involving youth leaders in community planning not only gets youth involved, but also has led to sustained funding for youth planning.
Linking Adolescents at Risk to Mental Health Services Grant Program
The Adolescents at Risk grant program provided funding to evaluate and document voluntary school-based suicide prevention programs being implemented in high schools. Its primary objective was to determine the extent to which these programs lead to successful referrals for treatment and other sources of help or the extent to which families are engaged in and accept the programs. All activities undertaken as part of this program were developed with respect to the ages of the adolescents, their cultural backgrounds, and the cultural backgrounds of their parents, legal guardians, and other caregivers.
Campus Suicide Prevention Grant Program
The Campus Suicide Prevention grant program provides funds to institutions of higher education to prevent suicide and suicide attempts and to enhance services for students who may experience academic challenges due to mental and behavioral health problems such as depression or substance abuse.
Activities funded by the program include:
- Providing gatekeeper training for students and campus personnel;
- Conducting educational seminars related to suicide;
- Creating informational materials for campus personnel and students and their families;
- Operating local hotlines or promoting the National Suicide Prevention Lifeline; and
- Increasing student access to mental health services on campus or in the community.
Summaries of individual campus programs are available through the SPRC at http://www.sprc.org/grantees/campus/desc/C_Udescriptions.asp.
Suicide Prevention Resource Center
The SPRC is a congressionally mandated, federally funded grant program that is managed through SAMHSA. The primary services offered by SPRC are to:
- Support the technical assistance and information needs of SAMHSA’s State and Tribal Youth Suicide Prevention and Early Intervention and Campus Suicide Prevention grantees and associated programs;
- Develop and conduct training on prevention products, materials, services, and strategies;
- Assist States, Territories, and Tribes in their efforts to plan for the development, implementation, and evaluation of suicide prevention programs;
- Collect and distribute information on best prevention practices;
- Facilitate informational exchanges and peer-to-peer mentoring using listservs and other technologies;
- Support the field of suicide prevention by developing and providing access to needed resources for implementing a public health approach; and
- Promote suicide prevention as a component of mental health transformation.
In addition to the Best Practices Registry described in the previous chapter, services and resources available from the SPRC include
the following.
- Prevention support: Prevention specialists are available to assist the suicide prevention efforts of State and Tribal suicide prevention coalitions and other agencies and organizations. These specialists can be consulted by telephone, e-mail and, in some situations, are available for presentations and training at meetings and conferences.
- SPRC Training Institute: The SPRC Training Institute offers an array of training programs, including a 1-day
workshop for mental health professionals on assessing and managing suicide risk, periodic Web-based seminars (Webinars) to foster dialog on a variety of topics, and a series of self-paced online workshops about youth suicide prevention. A free online workshop, “Planning and Evaluation for Youth Suicide Prevention,” is available at http://training.sprc.org. - Customized information: Each customized page provides information on recognizing and responding to the warning signs of suicide, resources, and other information chosen for its relevance to a particular audience (including parents, teens, first responders, and attempt survivors).
- Online library: The online library is a searchable collection of Web-based resources, including data, State prevention plans, and information on interventions, funding, grant-writing, planning and evaluation, and public education.
- Suicide prevention news: This compilation of news, funding opportunities, and abstracts of selected research articles is updated weekly. A news archive also is available.
- SPRC mailing list: Individuals who sign up for the SPRC mailing list will receive the Weekly Spark, a newsletter with updates on current news and other resources, as well as other occasional announcements.
Additional information about the SPRC is available from:
SPRC/EDC
55 Chapel Street
Newton, MA 02458-1060
Phone: 617–618–2572 or
1–877–GET-SPRC (1–877–438–7772)
(toll-free)
http://www.sprc.org
SPRC and State Resources
The SPRC Web site also provides links to individual State suicide prevention plans and data sheets, which can inform AI/AN
communities about local activities, service gaps, and opportunities for funding and collaboration. SPRC maintains a complete listing of State planning team leaders and contact information. A printed copy of this list is included in Appendix D: Decision-making Tools and Resources.
National Suicide Prevention Lifeline
SAMHSA’s National Suicide Prevention Lifeline initiative is aimed at crisis centers that respond to callers in extreme emotional crisis. Crisis center workers listen to callers, assess the nature and severity of their crisis, and link or refer callers to services. Accurate assessment and response can be life-saving.
The goals of this initiative are to:
• Enhance the training of crisis workers;
• Increase the number of crisis centers that are certified in crisis intervention;
• Improve crisis center referrals and follow through on referrals; and
• Encourage a consistent and clinically accepted approach for callers who appear to be at imminent risk of suicide.
Certified crisis centers are linked together through the National Suicide Prevention Lifeline at 1–800–273–TALK (8255). Telephone technology enables anyone in the United States who is in crisis to call this number and be forwarded to the closest crisis center. As a result of this initiative, there now are more than 140 certified crisis centers in the national network.
To ensure that veterans in emotional crisis have round-the-clock access to trained professionals, the U. S. Department of Veterans Affairs (VA) operates a hotline for veterans in partnership with SAMHSA and the National Suicide Prevention Lifeline. Veterans can call 1–800– 273–TALK (8255) and press “1” to reach the Veterans Suicide Prevention Hotline, which is staffed by mental health professionals.
The National Suicide Prevention Lifeline initiative provides organizations and communities with resources to make the public more aware of suicide and the help that is available through the Lifeline. For example, SAMHSA has wallet cards and brochures
that list the warning signs of suicide. Items such as these can be distributed in community centers, school-based counseling centers, and other locations where they will be available to young people contemplating suicide and to those who may be concerned that someone they know may need help. Most materials, such as the poster developed for AI/AN communities, can be customized by adding the logos and contact information for local collaborating organizations.
The Lifeline also offers publications for local distribution, such as a series of brochures for attempt survivors and those who care for them, including:
- After an Attempt—A Guide for Taking Care of Yourself After Your Treatment in the Emergency Department;
- After an Attempt—A Guide for Taking Care of Your Family Member After Treatment in the Emergency Room; and
- After an Attempt—A Guide for Medical Providers in the Emergency Department Taking Care of Suicide Attempt Survivors.
Although most Lifeline materials were developed for the general public, they provide valuable information for AI/AN communities. SAMHSA encourages these communities to adapt the materials and provide feedback to SAMHSA (Division of Prevention, Traumatic Stress, and Special Programs, Suicide Prevention Branch, 1 Choke Cherry Road, Rockville, MD 20857) on the need for and content of materials specially designed for their members.
Appendix E: Web Site Resources and Bibliography includes a complete listing of resources available through the National Suicide Prevention Lifeline and ordering information. Orders can be placed online at http://www.samhsa.gov/shin or by calling SAMHSA’s Health Information Network at 1-877-SAMHSA-7 (1-877-726-4727). All orders are free.
The National Suicide Prevention Lifeline reaches out to new media users through a variety of social networking sites. Its online Lifeline Gallery: Stories of Hope and Recovery (http://www.lifelinegallery.org) is a safe space for survivors of suicide, suicide attempt survivors, those who struggled with suicidal thoughts, and those in the suicide prevention field to share their stories of hope and recovery.
National Suicide Prevention Lifeline Initiative for AI/AN Communities
Providing access to AI/AN communities remains a Lifeline challenge. For some communities, phone service is lacking and the community has limited resources to start a crisis center. There also are cultural concerns. Off-reservation service providers may be unfamiliar with Tribal culture, and on-reservation service providers may feel constrained from taking action by issues of confidentiality.
In 2006, SAMHSA initiated a pilot program to enhance Lifeline access in Indian Country. Lifeline crisis centers in Montana, Wyoming, Minnesota, North Dakota, and South Dakota participated in the pilot. Objectives of the pilot program were to:
- Facilitate relationships between crisis center staff and stakeholders in Tribal communities;
- Develop cultural awareness and sensitivity training for crisis workers that serve a designated community;
- Strengthen the effectiveness of the local referral systems;
- Promote culturally sensitive social marketing and educational materials for Tribal communities; and
- Identify lessons learned from the pilot initiative for wider application to other AI/AN communities.
SAMHSA also is working collaboratively with IHS to promote the Lifeline nationwide in Indian Country.
Additional information about SAMHSA’s Lifeline initiative for AI/AN communities is available from:
Lifeline/Link2Health Solutions
Project Director
50 Broadway, 19th Floor
New York, NY 10004
Phone: 212–614–6357
http://www.suicidepreventionlifeline.org
Indian Health Service Resources
The following resources are available through the IHS, in support of its mission to raise the physical, mental, social, and spiritual health of AI/ANs to the highest level.
IHS National Suicide Prevention Initiative
The IHS has sponsored a National Suicide Prevention Initiative since 2003. This initiative:
- Builds on the goals and objectives of the National Strategy for Suicide Prevention;
- Strives to ensure that its efforts honor and respect AI/AN traditions and practices;
- Acknowledges the role and wisdom of Elders and spiritual leaders in healing and wellness; and
- Works to create collaborative, holistic, culturally appropriate efforts between AI/AN communities, government agencies, and nonprofit organizations in order to prevent suicide effectively.
The IHS has made substantial progress in planning and delivering suicide prevention programs, but recognizes that this is just the
beginning of a long-term, concerted, and coordinated effort among Federal, Tribal, State, and local community agencies. National
coordination and leadership is required for the development of resources, data systems, and promising programs, as well as sharing information across the system.
As a result, the IHS initiative focuses on three approaches:
- Assist IHS, Tribes, Tribal organizations, or urban Indian organizations (I/T/Us) in addressing suicide through cultural approaches at the community level;
- Strengthen and enhance IHS’ epidemiological and research capabilities in the areas of suicide and suicide prevention; and
- Promote collaboration between I/T/Us regarding suicide prevention.
To guide overall IHS/Tribal efforts under the initiative, the IHS has established a National Suicide Prevention Committee (SPC). Members of the SPC represent affected AI/AN communities through a variety of clinical professions, including therapists, psychologists, psychiatrists, agency administrators, injury prevention specialists, social workers, and traditional practitioners from a broad geographic distribution and from mixed IHS, Tribal, and urban settings. It is the responsibility of the SPC to provide recommendations and guidance to the IHS regarding suicide prevention and intervention in Indian Country.
SPC efforts include the development of an IHS National Suicide Prevention Strategic Plan and the development of Guidelines for Responding to I/T/U Requests for Assistance. The IHS National Suicide Prevention Strategic Plan is a first step in describing and promoting the accumulated practice-based wisdom in AI/AN communities. At its best, the plan will be a living and constantly changing reflection of the collaborative and focused efforts of the many people throughout AI/AN communities who are working to reduce suicide. The response guidelines will establish procedures and responsibilities for responding to requests for assistance from I/T/U organizations in the area of suicide prevention.
The IHS Suicide Prevention Initiative is complemented by the IHS Behavioral Health Initiative, which also seeks to address suicide
prevention through a holistic, community centered approach. Two other focus areas that are closely linked to the Behavioral Health Initiative are the IHS Chronic Disease Management and Health Promotion and Disease Prevention Initiatives. All three of these initiatives are pertinent to suicide prevention efforts and seek to address the underlying causes of poor physical and mental health rather than just treat the symptoms. They also stress the empowerment and full engagement of individuals, families, and communities in their own health care.
IHS Community Suicide Prevention Web Site
IHS maintains a Community Suicide Prevention Web site to provide AI/AN communities with culturally appropriate information about best and promising practices, training opportunities, and other relevant information regarding suicide prevention and intervention. This site is an information portal in that it does not list existing suicide prevention programs but, instead, links users to the sites of program developers and to current research articles. The goal of the Web site, at http://www.ihs.gov/NonMedicalPrograms/nspn, is to provide Native communities with the tools and information to create or adapt their own suicide prevention programs.
Additional information about the IHS Suicide Prevention Initiative and the Community Suicide Prevention Web site is available from:
Indian Health Service Headquarters
Office of Clinical and Preventive Services
801 Thompson Avenue, Suite 300
Rockville, MD 20852
E-mail: http://www.ihs.gov/NonMedicalPrograms/nspn
Additional resources and information about local IHS activities may be available through IHS area offices. Contact information follows. You also can find a current listing at http://www.ihs.gov/FacilitiesServices/AreaOffices/AreaOffices_index.asp.
IHS Regional Area Offices
North Dakota, South Dakota, Iowa, and Nebraska
Aberdeen Area Indian Health Service
Office of Professional Services
115 4th Avenue, SE
Aberdeen, SD 57401
Phone: 605–226–7582
Fax: 605–226–7321
Alaska
Alaska Area Native Health Service
4141 Ambassador Drive, Suite 300
Anchorage, AK 99508-5928
Phone: 907–729–3686
Fax: 907–729–3689
New Mexico, Colorado, and portions of Texas
Albuquerque Area Indian Health Service
5300 Homestead Road, NE
Albuquerque, NM 87110
Phone: 505–248–4500
Fax: 505–248–4115
Indiana, Minnesota, Michigan, and Wisconsin
Bemidji Area Indian Health Service
522 Minnesota Avenue, NW, Room 119
Bemidji, MN 56601
Phone: 218–444–0458
Fax: 218–444–0461
Montana and Wyoming
2900 4th Avenue North
Billings, MT 59101
or
P.O. Box 36600
Billings, MT 59107
Phone: 406–247–7248
Fax: 406–247–7230
California and Hawaii
California Area Indian Health Service
650 Capitol Mall, Suite 7–100
Sacramento, CA 95814
Phone: 916–930–3927
Fax: 916–930–3952
Eastern United States and portions of Texas
Nashville Area Indian Health Service
711 Stewarts Ferry Pike
Nashville, TN 37214-2634
Phone: 615–467–1500
Fax: 615–467–1501
Arizona, New Mexico, and portions of Utah
Navajo Area Indian Health Service
P.O. Box 9020
Window Rock, AZ 86515
Hwy. 264 and St. Michael Road
St. Michael, AZ 86511
Phone: 928–871–5811
Fax: 928–871–5866
Oklahoma, Kansas, and portions of Texas
Oklahoma City Area Indian Health Service
701 Market Drive
Oklahoma City, OK 73114
Phone: 405–951–3820
Fax: 405–951–3780
Arizona, Nevada, and portions of Utah
Phoenix Area Indian Health Service
Two Renaissance Square
40 North Central Avenue
Phoenix, AZ 85004-4424
Phone: 601–634–5039
Fax: 601–634–5042
Idaho, Oregon, and Washington
Portland Area Indian Health Service
1220 SW Third Avenue, #476
Portland, OR 97204
Phone: 503–326–2020
Fax: 503–326–7280
Southern Arizona
Tucson Area Indian Health Service
7900 S. J. Stock Road
Tucson, AZ 85746-7012
Phone: 520–295–2405
Fax: 520–295–2602
Other Federal Resources
Support for prevention programs that reduce suicide risk factors may be available from other Federal agencies, such as the online databases of prevention programs described in the previous chapter. Some agencies have funding available for prevention programs. Possible funding sources include the Office of Safe and Drug-Free Schools (OSDFS), part of the U.S. Department of Education, which funds school-based efforts that include projects designed to decrease drug involvement and youth violence. The Web site homepage for OSDFS is http://www.ed.gov/about/offices/list/osdfs/index.html.
The National Center for Injury Prevention and Control (NCIPC), part of the Centers for Disease Control and Prevention (CDC), offers extensive information about the nature of the problems of youth violence and youth suicide, both at the local and national levels, as well as funding opportunities for prevention research. There is a direct link to CDC funding initiatives on the NCIPC homepage at http://www.cdc.gov/ncipc.
The Office of Juvenile Justice and Delinquency Prevention (OJJDP), U.S. Department of Justice, has as a focus the prevention of juvenile delinquency and victimization. Possible support for community-based prevention efforts may be identified by visiting http://ojjdp.ncjrs.org and clicking on “funding” or “programs.” The Title V Community Prevention Grants Program, for example, funds collaborative, community-based delinquency prevention efforts designed to reduce risk factors associated with juvenile
delinquency and decrease the incidence of juvenile problem behavior. Many risk factors associated with juvenile delinquency, such as excessive exposure to violence, family disharmony, and school dropout, also are risk factors for suicide. Similarly, protective factors that help youth avoid delinquency and suicide, such as strong family bonds, are shared.
U.S. Federal/Canada Collaboration
In 2003, the U.S. Department of Health and Human Services and Health Canada first signed a Memorandum of Understanding (MOU) to promote the health of AI/ANs in the United States and First Nations people and Inuit in Canada. A direct outcome of the MOU is the Ad Hoc Working Group on Suicide Prevention. The purpose of the working group is to make it easier for the countries to share knowledge about suicide prevention and intervention and the relationship of alcohol abuse to suicidal behavior. Working group activities may include the exchange of personnel as well as information and the hosting of workshops, conferences, seminars, and meetings.
The two government agencies renewed the MOU in 2007. Since then, Health Canada has launched its youth suicide prevention Web site, at http://honouringlife.ca. This trilingual Web site (English, French, and Inuktitut) provides a place for Aboriginal youth to read about others dealing with similar issues and for those working with Aboriginal youth to connect, discuss, and share suicide prevention resources and strategies.
Conclusion
SAMHSA has established a clear vision for its work—a life in the community for everyone. To realize this vision, SAMHSA is gearing all of its resources—programs, policies, and grants—toward that outcome.
SAMHSA currently maintains four suicide prevention programs that directly or indirectly serve AI/AN youth and young adults: State and Tribal Youth Suicide Prevention and Early Intervention, Native Aspirations, Linking Adolescents at Risk for Suicide to Mental Health Services, and Campus Suicide Prevention. Regardless of whether a community has one of these grants, its members can access planning, implementation, and evaluation support through SAMHSA’s SPRC. Additional services and resources that encourage individuals experiencing an emotional crisis to seek help are available through the National Suicide Prevention Lifeline.
SAMHSA’s prevention efforts aimed at AI/AN communities are still evolving as new information and opportunities become available. For example, SAMHSA is exploring the potential of using telepsychiatry to make mental health care more accessible to residents, including AI/ANs, living in remote and underserved areas. An overarching goal of all of these efforts is to develop a better knowledge base of what works best in promoting mental health and preventing mental illnesses and suicide among AI/ANs. To achieve this goal, collaboration and information sharing among AI/AN communities and the organizations and government agencies involved is necessary. Breaking the code of silence around suicide is one crucial step forward in helping AI/AN youth and young adults on their path toward a mentally healthy and promising future. Communities have a variety of resources to draw
from after taking this first step.